Reducing the burden of malaria in children under five years of age in Cameroon

In 2016, eBASE Africa worked with the District Health Service of Bali in Cameroon to promote the use of research evidence in clinical practice for malaria, using JBI's evidence-based audit and feedback approach. Since then, malaria case management in the Bali District has seen the number of complicated malaria cases reduce by 78% over three years, with 233 complicated cases reported in 2016 compared with just 51 complicated cases in 2019. This is mainly due to more uncomplicated cases being correctly managed according to best evidence-based practice before complications set in.
Malaria is a deadly disease caused by parasites that are transmitted through mosquito bites. The 2019 WHO Malaria report estimated that 13,500 people died from malaria in Cameroon in 2018. Deaths from malaria usually result from complicated malaria; complicated malaria itself is a result of poorly managed uncomplicated malaria.
In 2016, JBI sponsored Dr Patrick Okwen to participate in the JBI Evidence Implementation Training Program (Formerly Evidence-based Clinical Fellowship Program) in order to equip him with the skills, knowledge and support to improve the management of uncomplicated malaria in Bali, Cameroon. As part of the program, participants develop an evidence-based implementation project to improve health outcomes in their clinical settings.
‘The program builds capacity in the use and implementation of research evidence and clinical leadership, and provides access to evidence summaries, audit criteria and evaluation software. It’s also an amazing opportunity for cultural exchange’, says Dr Okwen. ‘During the program, I spent four weeks in Adelaide with colleagues from eight different resource-limited settings learning and sharing skills, tips, and tricks on getting research evidence into practice, improving workplace culture and managing behaviour change. Apart from the many lessons we learnt from each other in relation to clinical practice, we also made good friends – we still get in touch with each other on WhatsApp to say “so far so safe” from the COVID-19 pandemic.‘
Dr Okwen’s implementation project aimed to promote evidence-based practice in artemisinin-based combination therapy (ACT) for managing uncomplicated malaria in children under five to improve patient outcomes and resource utilisation in the Bali Health District
‘The WHO recommends the use of ACT for the treatment of malaria. ACT has proven efficacy – it has been shown to significantly reduce morbidity and mortality – and it has good tolerance’, says Dr Okwen.
The project commenced with engaging stakeholders, establishing a team and conducting a baseline audit in three health units in the Bali Health District. Data such as hospital records, patients case notes, laboratory reports and pharmacy reports were used to measure compliance against five evidence-informed criteria:
1. Microscopy or rapid diagnosis test (RDT) is used to confirm the diagnosis in all suspected cases of malaria.
2. Antimalarial treatment is prescribed to patients on confirmation by positive microscopy and RDT.
3. Children with uncomplicated malaria are treated with ACT.
4. A three-day ACT treatment regimen is prescribed.
5. ACT is prescribed in cases of mixed malarial infections.
All criteria scored below 60% in the baseline audit, with one criterion scoring 1%. ‘Criterion 5 scored very poorly. RDTs, while being easy to use, only detect P. falciparum. The audit results for this criterion indicate that clinicians rarely test for mixed infections.’
Following the baseline audit, results were discussed with stakeholders in the health district, and consultations took place to determine the approach for influencing and managing practice change.
‘Together we identified barriers and facilitators to evidence implementation and identified interventions that are feasible, appropriate, meaningful and effective, and which will improve clinical care using the JBI GRiP (Getting Research into Practice) approach.’
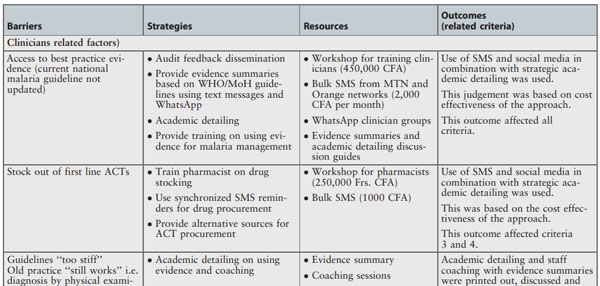
Strategies to overcome barriers included educating and resourcing lab technicians to encourage them to perform microscopy, given the inability of RDTs to distinguish between falciparum species. This meant that mixed malaria could be detected and treated.
Other barriers included parents’ lack of knowledge about the symptoms and management of malaria in children. As a result, an education campaign using talkback radio, social media and SMS was employed.
A follow-up audit at all three health centres was conducted as part of phase 3 of the project and demonstrated the project’s success across the three health centres. The aggregated results showed the following improvements in compliance against the evidence-informed criteria:
1. Microscopy or rapid diagnosis test (RDT) is used to confirm the diagnosis in all suspected cases of malaria: improved from 58% to 86%.
2. Antimalarial treatment is prescribed to patients on confirmation by positive microscopy and RDT: improved from 40% to 84%.
3. Children with uncomplicated malaria are treated with ACT: improved from 49% to 83%.
4. A three-day ACT treatment regimen is prescribed: improved from 53% to 93%.
5. ACT is prescribed in cases of mixed malarial infections: improved from 1% to 18%.
Overall, the follow-up audit conducted in December 2017 improved compliance with best practice by 31% across the three health centres. The audit also showed that patient record-keeping and documentation had improved significantly: ‘In the baseline data collection, we recorded 118 missing patient data while in the follow-up audit, we only recorded 58 missing patient data.’
As part of the continuous improvement process, another audit was conducted at all three health centres in 2018 and showed that compliance with best practice had improved from 31% to 96.3%. By April of 2019, the national DHIS2 database was reporting Bali as a model district in the case management of malaria in Cameroon, despite the ravaging armed conflict in the region. In order to maintain compliance with best practice over the past three years, the project team ensured staff were committed to evidence-based practice through regular feedback sessions at district-level coordination meetings. Using the health district as point of entry was helpful in ensuring that roll-out in other health facilities was possible.
‘The project demonstrates that local leadership and evidence-based care can significantly improve practice in resource-limited settings. As a primary care clinician, I believe the JBI approach to evidence implementation is my best bet to improve clinical effectiveness, improve quality of care, and change workplace culture’ says Dr Okwen.
Further Resources
Artemisinin based combination therapy for uncomplicated malaria management among children under five in Cameroon: a best practice implementation project
Effective Base Services (eBASE), Africa
JBI Manual for Evidence Implementation (for GRiP approach)
Author
Okwen Patrick1, Ngem Bedes2
1. Effective Basic Services (eBASE) Africa,
2. Ministry of Public Health, Cameroon

Disclaimer
The views expressed in this this World EBHC Day Impact Story, as well as any errors or omissions, are the sole responsibility of the author and do not represent the views of the World EBHC Day Steering Committee, Official Partners or Sponsors; nor does it imply endorsement by the aforementioned parties.