Integrating voices, integrating care: The G-SCOPE journey in family planning
Introduction
Family planning is central to improving women’s health, advancing gender equality and achieving universal health coverage and the UN’s Sustainable Development Goals. Global initiatives such as FP2030 have repeatedly emphasised the need to integrate family planning into broader health services. Despite this momentum, many women in low- and middle-income countries continue to experience fragmented care. A mother may attend an immunisation visit or a postnatal check-up but leave without contraceptive counselling. These missed opportunities highlight not just technical barriers but also failures in how knowledge is communicated and acted upon across health systems.
This year’s World Evidence-Based Healthcare (EBHC) Day, with its theme of collaborative knowledge communication, invites us to reflect on how evidence moves into practice, how trust in health services is built and how diverse voices can be included in shaping solutions. My research journey, which included a scoping review of global integration strategies, a forthcoming policy analysis of national documents from Pakistan, Ethiopia and Kenya, case studies with providers and communities and an organisational study in Australia, sought to explore these very issues.
The outcome was the G-SCOPE Framework, an evidence-informed and co-created model for strengthening family planning integration. By combining research, policy insights, provider perspectives and women’s experiences, it reflects the campaign’s call to value multiple ways of knowing. This blog shares how G-SCOPE responds to persistent gaps in integration and illustrates why collaborative knowledge communication is essential for creating equitable, trusted and sustainable health systems.
Background
Despite global commitments, the integration of family planning into broader health systems has remained uneven, as highlighted in a scoping review of integration across LMICs and in a forthcoming analysis of national policies from Pakistan, Ethiopia and Kenya. In many LMICs, services are delivered in silos, with family planning often managed separately from maternal health, HIV care or child health. This fragmentation creates inefficiencies and duplicates effort, leaving women without access to contraception during routine visits. For example, studies in Kenya and Uganda have shown that women attending child immunisation or postnatal services were rarely offered family planning, leading to what researchers call ‘missed opportunities for care.’
Evidence from the Integrating Family Planning into Health Services project has demonstrated that integration can improve efficiency, continuity and client satisfaction by meeting several needs in a single encounter. However, assessments of facility readiness in Ethiopia and Nigeria report shortages of trained staff, inadequate counselling spaces and weak referral systems, making it difficult for integration to succeed. Evaluations of contraceptive programs in Malawi and Tanzania have documented frequent stock-outs, undermining women’s trust and discouraging continuity of use. Providers interviewed during my forthcoming case studies in Pakistan and Ethiopia also described how lack of supplies undermined their ability to meet demand.
Community perspectives highlight how stigma, myths and lack of confidentiality limit family planning access, with studies from South Asia and sub-Saharan Africa showing these barriers particularly affect adolescents and marginalised groups.
These realities suggest that integration cannot succeed through technical fixes alone. Progress depends on whether knowledge is communicated and acted upon across all levels of the system, from policymakers and providers to communities themselves and on whether diverse forms of evidence and experience are valued equally. These insights shaped the development of the G-SCOPE Framework, designed to help translate commitments into practice and make family planning integration more sustainable and people-centred.
The problem
Weak integration of family planning into health systems has lasting consequences for women and communities. Missed opportunities during routine visits, such as immunisation or post-abortion care, leave women without essential information or services, fuelling high levels of unmet need and unintended pregnancies. These consequences highlight a persistent gap between knowledge and practice, raising critical questions about how health systems can communicate evidence effectively, maintain trust in services and ensure inclusivity for adolescents and marginalised groups. Without stronger approaches, integration remains fragmented and the promise of comprehensive, people-centred care in low-resource settings is left unfulfilled.
The search for answers and G-SCOPE Framework
Building on evidence and experience
To address the persistent gaps in family planning integration, I embarked on a research journey that led to the development of the G-SCOPE Framework. This began with a scoping review of global strategies, which showed that integration improved efficiency and client satisfaction but was often limited by weak facility readiness, stock-outs and poor community engagement. I then carried out a policy analysis of national documents from Pakistan, Ethiopia and Kenya and conducted case studies with providers and communities. Each stage added insights, from global evidence to national commitments and lived experiences.
The outcome was the G-SCOPE Framework, designed as both a diagnostic tool and a guide for action. By combining research, policy insights, provider perspectives and community voices, it reflects the multiple ways of knowing that the World EBHC Day campaign emphasises as essential for stronger, more sustainable health systems.
The five pillars of G-SCOPE
The G-SCOPE Framework is built on five interconnected pillars that together make integration sustainable and people-centred.
1. Governance, policy alignment and stakeholder engagement provide the foundation for action. While many countries have ambitious policies, fragmented responsibilities create duplication and inefficiency. This pillar calls for coordinated leadership and inclusive platforms where policymakers, providers, donors and communities can align priorities.
2. Service delivery and readiness ensure integration is experienced at the point of care. Family planning should be part of routine visits such as antenatal, postnatal, immunisation, or HIV services. Embedding family planning into standard workflows reduces missed opportunities and makes care more responsive.
3. Commodity security and supply chain management are critical for maintaining trust. Frequent contraceptive stock-outs undermine both providers and clients. Reliable forecasting and distribution are essential to ensure that services are consistent and dependable.
4. Capacity-building and supportive supervision equip providers to act on evidence. Integration cannot succeed with one-off training or inspection-driven supervision. Continuous mentoring, learning and task-sharing give providers the confidence and support to deliver comprehensive care.
5. Public engagement and equity place communities at the centre. Stigma, myths and lack of confidentiality often discourage women and adolescents from seeking services. This pillar emphasises dialogue, youth-friendly approaches and feedback mechanisms that make services inclusive and trusted.
Together, these pillars strengthen the foundation for integration, ensuring that family planning is not a separate program but an essential part of comprehensive health care.
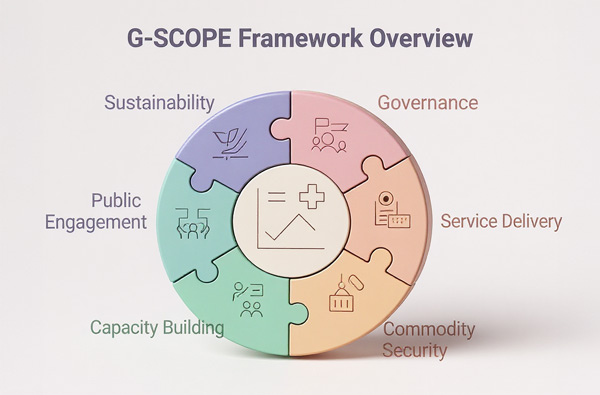
Figure: The G-SCOPE Framework shows five interconnected pillars with sustainability running across all of them.
The cross-cutting principle of sustainability
Sustainability runs across every pillar of G-SCOPE. Integration cannot be treated as a temporary donor project but must become part of the long-term transformation of health systems. This means embedding family planning into budgets, data systems and governance structures so that it is delivered routinely and reliably. Sustaining integration in this way reflects the campaign’s call to move beyond short-term, technical fixes toward approaches that genuinely strengthen health systems and respond to community needs over time.
Why G-SCOPE matters
The G-SCOPE Framework directly responds to the reflections raised by this year’s World EBHC Day campaign. It helps close the gap between evidence and practice by showing how commitments can translate into everyday services. It addresses uncertainty by emphasising readiness and consistent supplies, ensuring that trust in services is maintained. It promotes inclusivity by placing community voices at the centre and recognising that evidence, values and experiences are equally valid ways of knowing. And it fosters collaboration by bringing policymakers, providers and communities into the same conversation. More than a research product, G-SCOPE is a tool for communication, dialogue and action. It demonstrates how evidence can be shared in collaborative and creative ways, offering a pathway to family planning integration that is equitable, sustainable and people-centred.
Lessons from the journey
The process of developing and reflecting on G-SCOPE revealed several recurring challenges:
- Ministries often worked in silos and integration was sometimes driven by donor priorities rather than local needs.
- Health facilities were underprepared, with limited staff and resources, and integration was treated as an extra task instead of routine care.
- Contraceptive stock-outs weakened trust, underscoring the importance of reliable supply chains and better coordination.
- Training and supervision were inconsistent, leaving providers without adequate mentoring or support.
- Community voices were often excluded, while stigma and myths discouraged women and adolescents, highlighting the need for equity-focused engagement.
Next steps
The next step for G-SCOPE is to move into advocacy with governments in LMICs. The framework emphasises that evidence, policy judgement, provider expertise and community voices must come together to guide integration. Using creative approaches such as infographics, storytelling and dialogue, G-SCOPE will be shared as both a technical tool and a platform for collaboration, fostering global reflection on how integration strengthens health systems and advances universal health coverage.
Key take-home messages
The G-SCOPE Framework shows that family planning integration works best when evidence, policy judgement, provider expertise and community voices are valued equally. By strengthening governance, readiness, supply chains, provider support and community engagement, it helps close the gap between knowledge and practice. More than a technical tool, G-SCOPE is a process of collaborative knowledge communication, offering governments a practical way to build equitable, trusted and sustainable health systems.
References
Transforming our world: the 2030 Agenda for Sustainable Development | Department of Economic and Social Affairs. 2015. Available at: https://sdgs.un.org/2030agenda
‘FP2030’ (2021) Family Planning 2030. Available at: https://www.fp2030.org/about/
World Evidence-Based Healthcare Day 2025. World EBHC Day Campaign Website. Available at: https://worldebhcday.org/
Gul, F., Lassi, Z., Mahmood, A., et al. The process of integrating family planning services with other reproductive health services in low- and middle-income countries: a scoping review. International Journal of Integrated Care, 2024;24(2).
Available at: https://ijic.org/articles/10.5334/ijic.8912
Thiongo, M.N., Gichangi, P.B., Waithaka, M., et al. Missed opportunities for family planning counselling among postpartum women in eleven counties in Kenya. BMC Public Health 2022;22:253. https://doi.org/10.1186/s12889-022-12623-0
Pfitzer, A., Maly, C., Tappis, H., et al. Characteristics of successful integrated family planning and maternal and child health services: findings from a mixed-method, descriptive evaluation. F1000Research, 2020;8:229.
Titiyos, A., Mehretie, Y., Alemayehu, Y.K., et al. Family planning integration in Ethiopia's primary health care system: a qualitative study on opportunities, challenges and best practices. Reprod Health. 2023 Dec 1;20(1):176. doi: 10.1186/s12978-023-01709-6. PMID: 38041131; PMCID: PMC10693018.
Chipokosa, S., Pattnaik, A., NEP Malawi Technical Task Team, et al. How strong are Malawi's family planning programs for adolescent and adult women? Results of a national assessment of implementation strength conducted by Malawi's National Evaluation Platform. J Glob Health. 2019;9(2):020901. doi: 10.7189/jogh.09.020901. PMID: 33282227; PMCID: PMC7689283.
Gul, F., Lassi, Z.S., Tessema, G.A. et al. Integrating family planning with reproductive health services: A multi-case study protocol. Sexual Reprod Healthcare, 2025;44:101090.
Chandra-Mouli, V., Lane, C., Wong, S. What does not work in adolescent sexual and reproductive health: a review of evidence on interventions commonly accepted as best practices. Glob Health Sci Pract. 2015;3(3):333-40. doi: 10.9745/GHSP-D-15-00126. PMID: 26374795; PMCID: PMC4570008.
Mwaisaka, J., Gonsalves, L., Thiongo, M. et al. Exploring contraception myths and misconceptions among young men and women in Kwale County, Kenya. BMC Public Health 2020;20:1694. https://doi.org/10.1186/s12889-020-09849-1
To link to this article - DOI: https://doi.org/10.70253/ERYG3563
Links to Additional Resources
https://researchers.adelaide.edu.au/profile/farina.gul
Co-publication declaration
Gul, F., Lassi, Z., Mahmood, A., Tessema, G. (2024). The Process of Integrating Family Planning Services with Other Reproductive Health Services in Low- and Middle-Income Countries: A Scoping Review. International Journal of Integrated Care, 24(2).
Available at: https://ijic.org/articles/10.5334/ijic.8912
Gul, F., Lassi, Z.S., Tessema, G.A. and Mahmood, M.A., 2025. Integrating family planning with reproductive health services: A multi-case study protocol. Sexual & Reproductive Healthcare, 44, p.101090.
Disclaimer
The views expressed in this World EBHC Day Blog, as well as any errors or omissions, are the sole responsibility of the author and do not represent the views of the World EBHC Day Steering Committee, Official Partners or Sponsors; nor does it imply endorsement by the aforementioned parties.
