The effect of patient education on improving self-care for transplant patients

The National University Hospital (NUH) is a tertiary hospital and major referral centre with over 50 medical, surgical and dental specialities, offering a comprehensive suite of specialist care. It is the only public hospital in Singapore to offer a paediatric kidney and liver transplant programme, in addition to kidney, liver and pancreas transplantation for adults.
As an academic health institution, patient safety and good clinical outcomes are the focus of the hospital. The National University Hospital takes great pride in translating research evidence into practice and is at the forefront of advocating evidence-based nursing to influence positive clinical outcomes in Singapore.

The National University Hospital is also a JBI Centre of Excellence, and both institutions have partnered to offer the JBI Evidence Implementation Program (formerly Evidence-based Clinical Fellowship Program). Liaw Yi Qi, a senior staff nurse, attended the program to develop the knowledge and skills needed to champion practice change within the hospital. Through this program, she was inspired to implement interventions that could improve the self-care of transplant patients to foster independence in their transplant journey, and ultimately improve their health outcomes.
The amount of fluids taken by transplant patients often guides their care plans, and patients are required to chart their own fluid intake after discharge. However, the recording of fluid intake during the patients’ stay in hospital can sometimes be inaccurate. Additionally, as transplant patients are immunocompromised, they are highly susceptible to acquiring infections, and in particular urinary tract infections (UTIs). The lack of proper and standardised education on the collection of midstream urine needed to diagnose the bacteria responsible for UTIs resulted in contaminated samples that could not accurately guide the use of antibiotics and treatment plans for the patient.
“I am a firm believer in the use of evidence-based practice to transform patient care. I believe that wastage can be reduced through the application of validated interventions. Thus, in order to address these issues, I applied the principles that I learnt during the JBI Evidence-Based Clinical Fellowship Program”, says Liaw.
The JBI Practical Application of Clinical Evidence System (PACES) and Getting Research into Practice (GRiP) Audit and Feedback program were used for a six-month, evidence-based implementation project focused on improving patient education for transplant patients to enhance self-care practices. The JBI evidence summary indicated that the accuracy of charting patients’ fluid intake could be improved by involving patients in their own intake charting. To facilitate this, the project team created a patient intake chart.
This chart was given to patients immediately upon admission and nurses would educate patients on the importance of fluid intake charting and the various volumes of cups and bowls in the hospital. Once the patients were assessed as competent, they were expected to take charge of their own charting during their hospitalisation to form a habit that would continue after discharge. With this implementation, patient involvement rates increased from 3% at baseline audit to 87% at one-month post implementation audit and continued to sustain high levels of compliance (more than 80%) even after six months’ post implementation. Accuracy of fluid intake charting has continued to be sustained from the implementation of the project in 2018 to the present through standardised patient education and the use of the patient intake chart. This initiative has helped to foster independence and empowered patients through education and involvement.

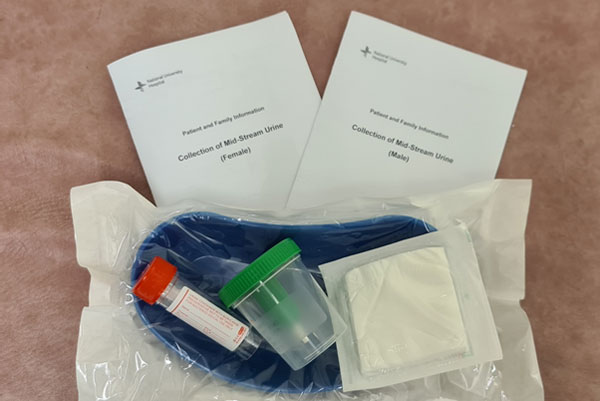
Evidence from JBI also suggested that patients should be educated by a healthcare professional before collecting their own midstream urine to ensure a clean sample for urinalysis. This led to the development of a patient education leaflet used as a standardised guide for nurses to educate patients and for patients to keep as a reference. The leaflet minimised confusion and prevented conflicting instructions from nurses to patients.
In addition, visual aids in the leaflet helped patients better understand the rationale and steps involved in collecting a clean midstream urine sample. The baseline audit demonstrated that there was a 40% contamination rate of midstream urine samples. One month after the implementation of the patient education initiatives, the contamination rate of midstream urine samples decreased to 26.7%, and after three-months it dropped even further to 20%.
The use of the patient education leaflet continues to this day and has been implemented into the surgical department’s patient education programme. Follow-up audits have recorded the sustained decrease in midstream urine sample contamination rates. This initiative demonstrated that optimal outcomes were more likely to be achieved by incorporating patient education into the patient’s plan of care.
During the initial phase of the project, ward nurses highlighted the lack of availability of both the patient intake chart and the education leaflet. As these initiatives were newly implemented, only the hard copy version was available, however, there was often a delay in accessing these. In response to feedback from nurses, the project team made soft copies available on point-of-care computers, which allowed nurses to print from whichever computer terminal they were on. This not only ensured the resources were available at all times, it was also easier for the nurses to gain quick access to the resources instead of having to rely on a single access point in the ward.
The success of the project can also be attributed in part to the positive attitudes of the nurses. They were extremely involved throughout the change process and were willing to adopt the new processes to help patients achieve better outcomes, even if it meant spending additional time on the new educational initiatives. They took ownership of the project, which ensured the sustainability of the interventions, and their eventual integration into guidelines and the daily practices of the ward.
“The practice changes not only help make nursing processes more efficient; patients also become more empowered, which helps us achieve the outcomes more effectively”, says Tiffany Ng, a registered nurse working in the implementation ward.
“With the continuous advancement of technology, patients and their families are no longer passive consumers in the healthcare paradigm. Patients increasingly want to play a greater role in managing their health conditions. Nurses should take this opportunity to engage in patient education and continue to innovate by seeking out new technologies to enhance the patient education process, which can lead to better outcomes and quality of care” says Liaw.
Further Resources
National University Hospital: https://www.nuh.com.sg/Pages/Home.aspx
Liaw YQ, Goh ML. Improving the accuracy of fluid intake charting through patient involvement in an adult surgical ward: a best practice implementation project. JBI Evid Synth. 2018;16(8):1709-19.
Liaw YQ, Goh ML. Reducing contamination of midstream urine samples through standardized collection processes: a best practice implementation project. JBI Evid Synth. 2020;18(1):256-71.
JBI Manual for Evidence Implementation (for GRiP approach)
Author
Liaw Yi Qi1,2
1. Nursing, National University Hospital, National University Health System, Singapore
2. Singapore National University Hospital (NUH) Centre for Evidence-Based Nursing, A JBI Centre of Excellence

References
Peters MDJ. Evidence summary. Urine sampling: midstream urine specimen. The Joanna Briggs Institute EBP Database. JBI@Ovid. 2017; JBI13874.
Disclaimer
The views expressed in this this World EBHC Day Impact Story, as well as any errors or omissions, are the sole responsibility of the author and do not represent the views of the World EBHC Day Steering Committee, Official Partners or Sponsors; nor does it imply endorsement by the aforementioned parties.